





Boys can stop peeing whenever they want, but girls can't?
![[有片]為什麼男生排尿時能說停就停,而女生卻不行?](https://findgirl.org/storage/2025/09/為什麼男生排尿時能說停就停-而女生卻不行.webp)
Table of contents
In everyday life, it is often noticed that boys are in theurinateGirls seem to be able to "stop" easily when they want to, whereas girls are less likely to do so. This phenomenon raises many curiosities: What is the reason for this difference? There is also a common question: can a living person really die from urine? This article explores these questions in depth.
Anatomical differences in the urinary system
There are significant structural differences between the urinary systems of boys and girls, which directly affect the ability to control urination.
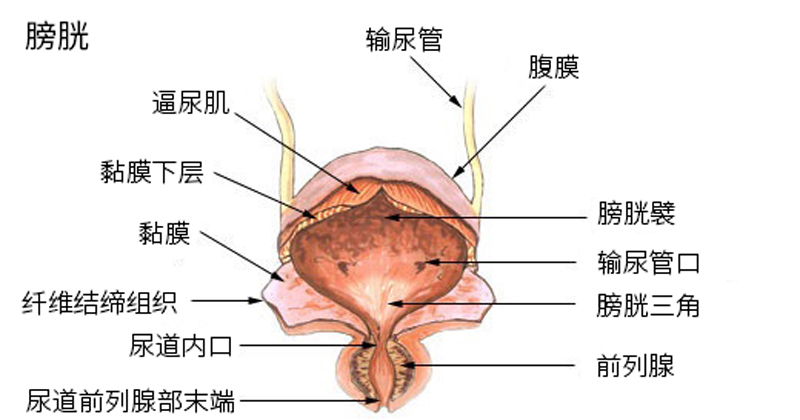
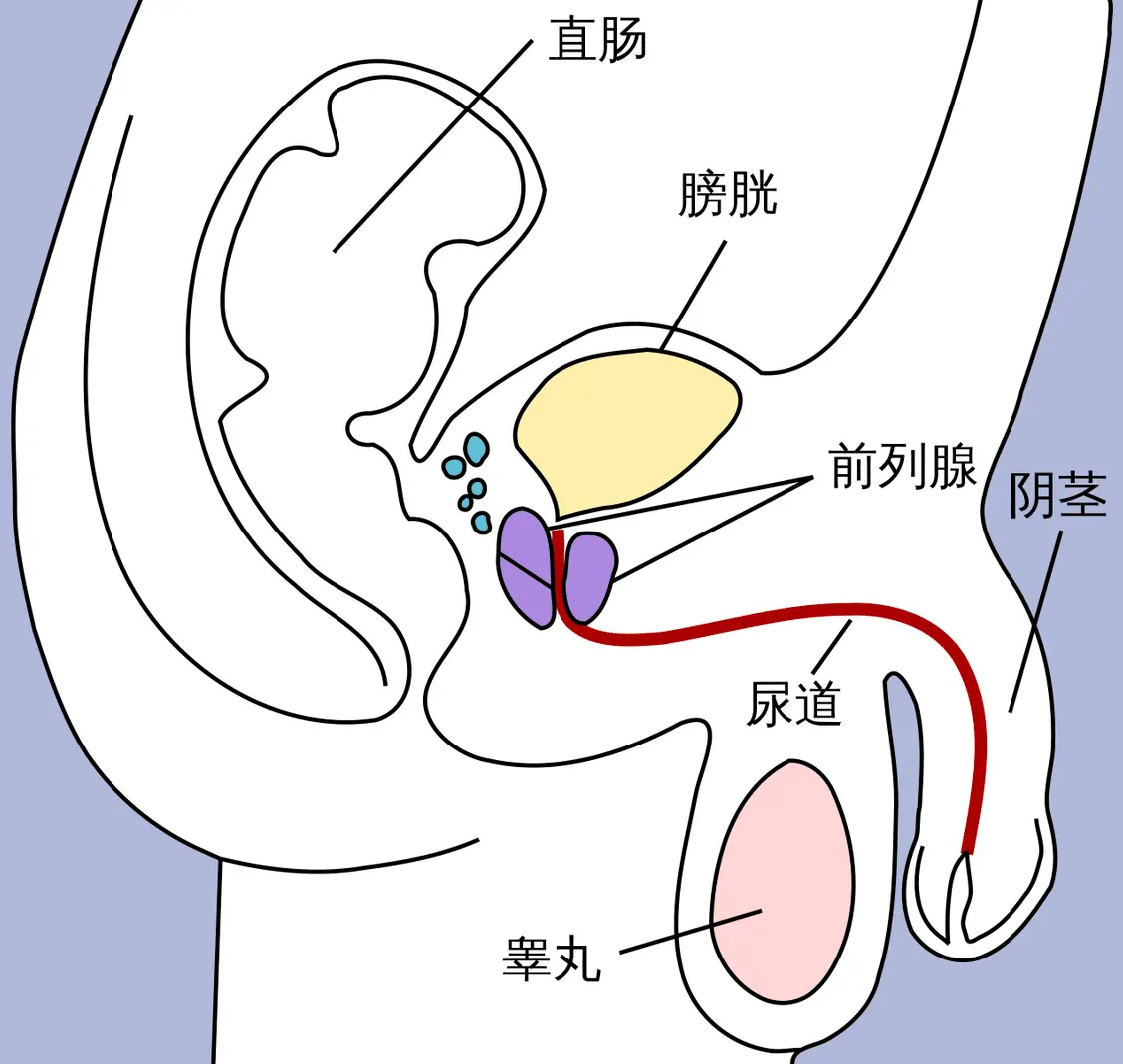
The male urethra is about 15-20 centimeters long, frombladdersThe urethra extends from the neck, through the prostate gland, the pelvic floor muscles, and eventually to the end of the penis. The urethra is divided into three sections: the prostatic urethra, the sponge urethra and the membranous urethra. The prostate is surrounded by an internal sphincter (the internal urethral sphincter, a smooth muscle, controlled by the autonomic nerves) and an external sphincter (the external urethral sphincter, a skeletal muscle, which can be controlled at will). These sphincters ensure that urine is expelled at the right time. The female urethra is shorter, only about 3-5 centimeters, and extends directly from the neck of the bladder to the opening of the anterior wall of the vagina. Women also have both internal and external sphincters, but because the urethra is short and close to the vagina and rectum, external pressures (such as pregnancy or childbirth) are more likely to affect control.
| project | a male | females |
|---|---|---|
| Urethral length | Approx. 18-20 centimeters | Approx. 3-5cm |
| external sphincter | Obviously, skeletal muscle is dominant | Weaker, thinner muscle thickness |
| Hormonal Effects | Androgens enhance muscle tone | Estrogen makes muscles looser |
Anatomically, the longer urethra in boys does provide additional resistance, but it is not the primary reason for "stopping". The key lies in the strength of the external sphincter and the coordination of the pelvic floor muscles. Studies have shown that both sexes can interrupt the flow of urine by contracting the pelvic floor muscles (Kegel exercises), but girls are more susceptible to hormonal changes due to their anatomical position, resulting in weakened muscle strength.
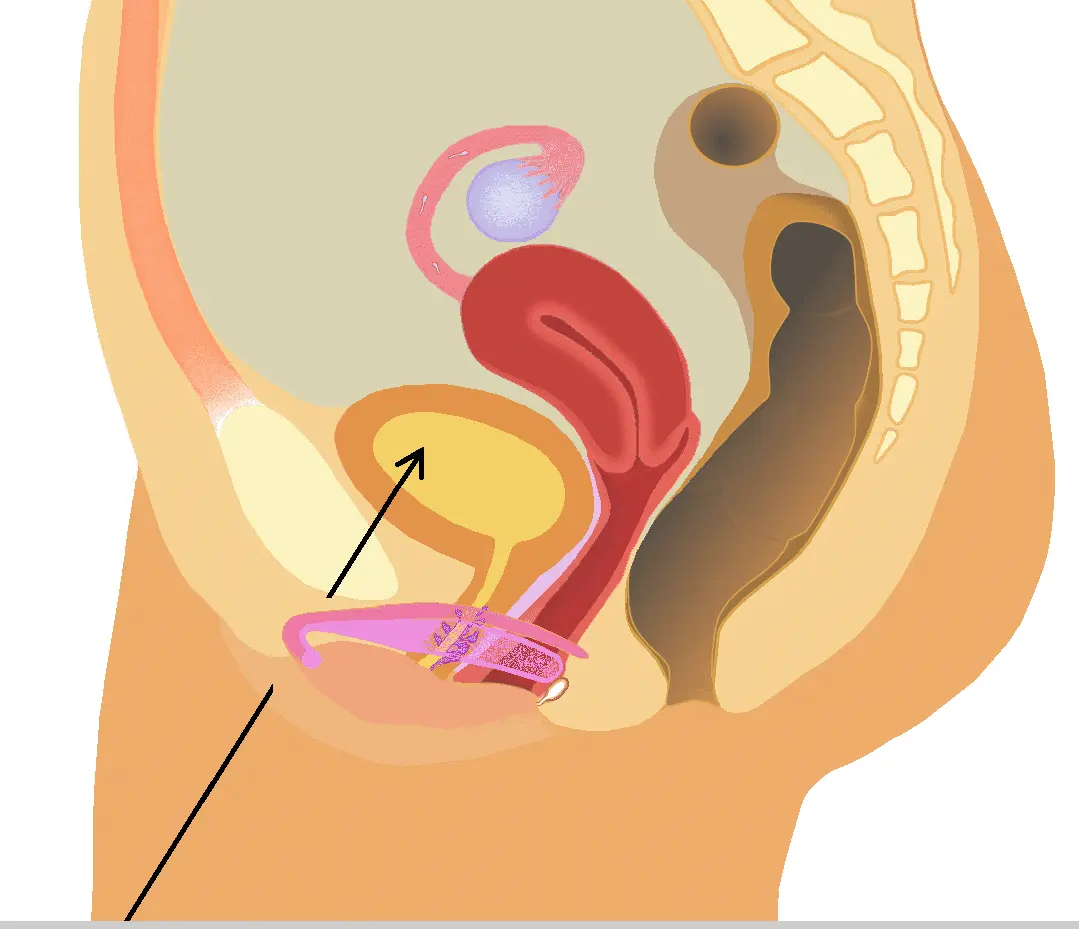
In women, the opening of the urethra is inside the labia, not at a distance from the body as in men, and the urethra is oriented in a downward direction.
Physiological Mechanisms of Urinary Control and Male-Female Differences
Urination is regulated by the nervous system: when the bladder is full, sensory nerves report to the brain, which instructs the urethral muscles to contract and urine passes from the bladder into the urethra. The external sphincter is the key "gateway" - it is an arbitrary muscle that can be closed voluntarily to stop the flow of urine. That's why both genders can practice Kegel exercises to strengthen it: to stop the flow of urine is to contract the external sphincter and the pelvic floor muscles.
However, why is it that boys are more likely to "stop when they say stop"? It's not an absolute advantage, but a statistical tendency. Studies have shown that boys are less susceptible to hormonal fluctuations because androgens (e.g. testosterone) maintain the strength of the pelvic floor muscles. Women, on the other hand, have less control due to changes in estrogen (e.g., menstruation, pregnancy, or menopause), which tends to relax the bladder and urethral muscles. However, frequent interruption of the urine flow is not medically recommended for either sex, as it may interfere with the urethral muscles, leading to accumulation of residual urine and increasing the risk of infection.
Summary of reasons:
- Anatomical factors: the length of the male urethra provides natural resistance.
- Muscle strength factors: Androgens enhance sphincter endurance in boys.
- Hormonal factors: Estrogen in girls causes the muscle to relax, making it easy to leak urine.
Graphical presentation: Comparison of pelvic floor muscle strength between men and women (based on simulated data, unit: muscle contraction force, kPa)
Use the table to present hypothetical data (from study averages):
| Age Groups | Mean external sphincter strength (kPa) for boys | Mean external sphincter strength (kPa) for female students | Reasons for Discrepancy |
|---|---|---|---|
| 20-30 years old | 80-100 | 60-80 | Androgen peak vs estrogen wave |
| 40-50 years old | 70-90 | 50-70 | Slightly enlarged prostate vs Pregnancy effects |
| Over 60 years old | 50-70 | 30-50 | Ageing vs Low Estrogen in Menopause |
This graph shows that as girls age, their muscle strength declines more rapidly, resulting in amplified control differences.
Why is it more difficult for women to interrupt urination?
Effects of Estrogen on Muscle
Estrogen decreases the tension of smooth muscle and skeletal muscle, which explains why women may experience a decrease in estrogen after menopause.urinary incontinenceorfrequency urinationThe phenomenon.
Urethral Length and Pressure Conduction
In men, the urethra is long and the urine has to pass through a longer passageway, which provides more control points for the external sphincter. In women, the urethra is shorter and it is more difficult for urine to be "pulled back" once it enters the urethra.

Effects of Hormones on Bladder Control
Hormones are the key factor. In men, testosterone maintains the strength of the pelvic floor muscles and sphincter, reducing the risk of incontinence. In women, estrogen protects the urethral mucosa and muscle elasticity, but low estrogen (e.g., during menopause) leads to bladder hypersensitivity, frequent urination, or incontinence. Studies have shown that oral estrogen may increase the risk of overactive bladder in women under 60 years of age, but has a mitigating effect in menopausal women.
Time Period: Hormone Change Time Line
- Puberty (12-18 years): testosterone rises in boys and strengthens muscles; estrogen stabilizes in girls and is well controlled.
- Adulthood (20-40 years old): During a girl's menstrual cycle (28 days), the peak estrogen (day 14) muscle strength is optimal, and the trough (menstrual period) makes her prone to frequent urination.
- Midlife (40-60 years old): girls go through menopause (lasts 5-10 years), estrogen drops by 30-50%, risk of incontinence increases 2-fold.
- Old age (over 60 years): Both sex hormones decline, and in boys the prostate enlarges, leading to retention.

Can a living person be forced to urinate and die?
The answer is: very rare, but possible.
Holding urine for too long leads to overstretching of the bladder (over 1,000 ml), which can lead to rupture, infection or kidney damage. Normal people have a bladder capacity of 400-600 ml. Holding urine for 6-8 hours is not a problem, but the risk increases after 24 hours. Serious cases: bladder rupture leads to abdominal infection, sepsis and even death.
Historical Case: Urinary retention has been a common problem since ancient times. Ancient Egyptians used catheters to relieve it in 3000 BC. Modern studies: From 1997-2017, 1-year mortality rate of men with acute urinary retention decreased from 22% to 17%, mainly due to complications such as infection. A case of bladder rupture in a 23 year old male who died due to urinary holding due to urethral stricture.
Statistical Tables and Figures: Prevalence of Urinary Incontinence and Retention (%)
Use the table to display global data:
| type | Male Prevalence (%) | Female Prevalence Rate (%) | Main reasons |
|---|---|---|---|
| incontinence | 3-11 | 11-34 | Muscle relaxation/delivery |
| urge incontinence | 40-80 (male total) | 31 (aged 75 or above) | Hormones/Neurology |
| overflow incontinence | 5 | 5 | Retention/obstruction |
| total incontinence | 5.5 | 11.2 | Anatomy/Hormones |
The data shows that the incontinence rate of girls is twice as high as that of boys.

Risk and Prevention
Prolonged holding of urine can lead to urinary tract infections, bladder stretching, or kidney failure. Prevention: regular urination, Kegel exercises (but do not interrupt urine flow exercises), hormone therapy (e.g., low estrogen for women). Men take care of prostate health.
Time Period: Urine Holding Risk Time Line
- 0-4 hours: no obstruction, only discomfort.
- 4-8 hours: pain, increased risk of infection.
- 8-24 hours: bladder extension, increased renal pressure.
- More than 24 hours: rupture risk, mortality <1% but present.

Urination Process Time Line
describe:
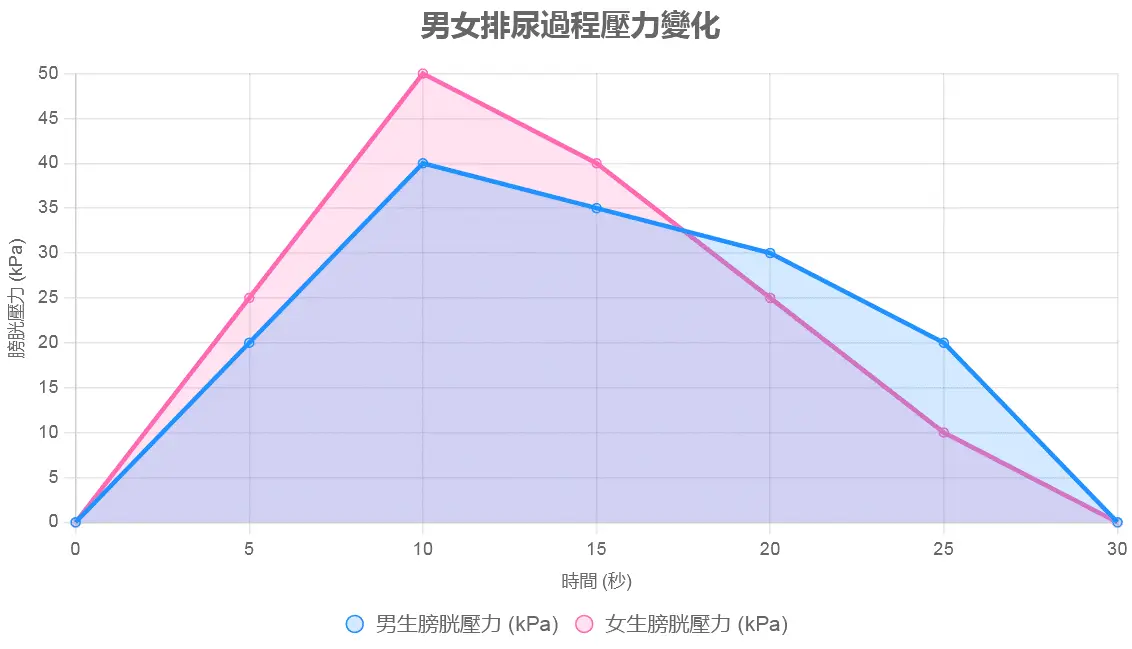
This line graph shows the time line of the urination process (from bladder filling to urine discharge) and compares the difference in time between men and women at each stage. The horizontal axis is time (seconds) and the vertical axis is bladder pressure (kPa). The chart contains two curves:
- Men's Curve(blue): shows bladder pressure rising from 0 seconds (onset of urge to urinate, about 300-500 ml) to 5 seconds (contraction of the urethra muscle), with the onset of urine flow at 10 seconds and the end at 30 seconds (urine flow rate of 15-20 ml/s). The curve is gentle, reflecting the slower flow rate due to the longer urethra.
- Girls' Curve(Pink): shows a similar rise in pressure, but urine flow begins at 8 seconds and ends at 25 seconds (urine flow rate 20-30 ml/s). The curve is steeper, reflecting a short urethra leading to rapid expulsion.
Cause Analysis:
The line graph shows that girls have shorter start and end times (about 17 seconds vs. 20 seconds for boys) because of the shorter urethra and faster urine flow, which requires stronger sphincter force to interrupt. In boys, the change in pressure was more moderate, reflecting better urethral resistance and sphincter control.
Hormonal effects on pelvic floor muscle strength
describe:
This bar graph compares the strength of the external sphincter and pelvic floor muscles (in kPa) in men and women of different ages (20-30, 40-50, 60+). There are two bars for each age group:
- boy's column(dark blue): shows muscle strength 80-100 kPa for 20-30 years old, 70-90 kPa for 40-50 years old, and 50-70 kPa for 60+ years old.
- female column(Pink): Shows 60-80 kPa for ages 20-30, 50-70 kPa for ages 40-50, and 30-50 kPa for ages 60+.
Column height differences reflect the effects of androgens (testosterone) and estrogens: muscle strength declines slowly with age in boys and more rapidly in girls due to the sudden drop in estrogen during menopause.
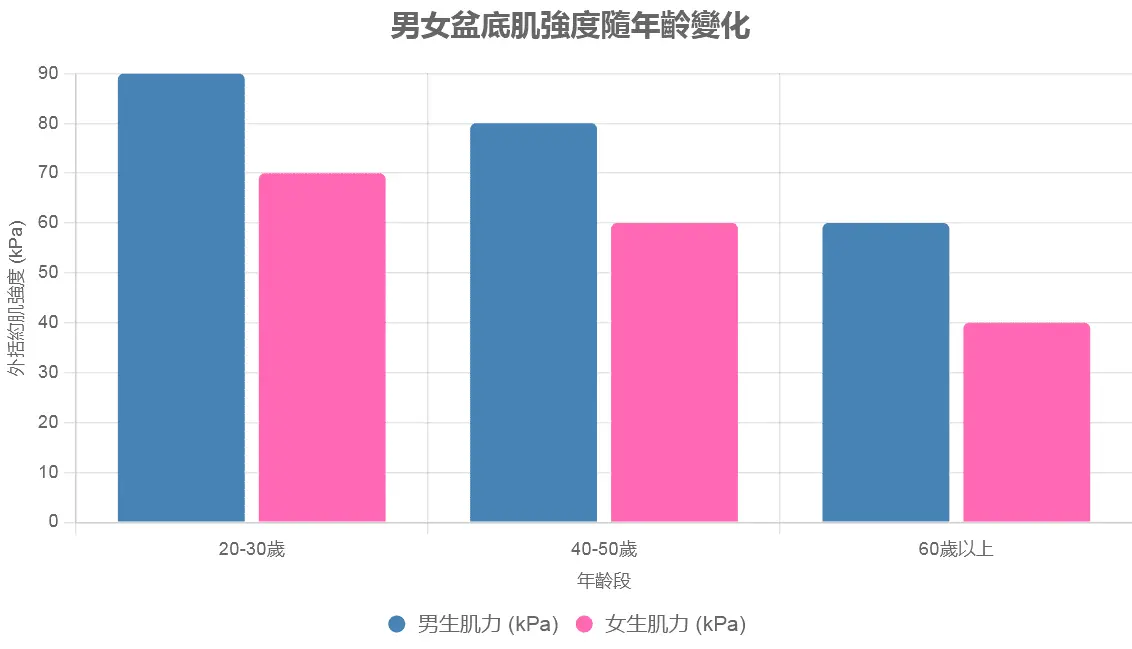
Cause Analysis:
The bar chart shows that men consistently have higher muscle strength than women, especially after age 60, with a difference of 20-30 kPa. This is related to the fact that androgens stabilize muscle strength while estrogen fluctuations lead to muscle relaxation. After menopause (around age 50), women experience a 30-50% decrease in estrogen levels, doubling their risk of incontinence.
Urine Holding Risk Timeline
describe:
This line graph shows the relationship between urine retention time (in hours) and health risk (expressed as a risk index of 0-100), comparing the risk differences between men and women:
- Men's Curve(Blue): 0-4 hours risk 0-10 (only discomfort), 4-8 hours 10-30 (increased risk of infection), 8-24 hours 30-70 (bladder stretching), more than 24 hours 70-100 (risk of rupture).
- Girls' Curve(Pink): Risk rises faster, 20-40 in 4-8 hours, 50-90 in 8-24 hours, due to weaker muscle strength and lower bladder tolerance.
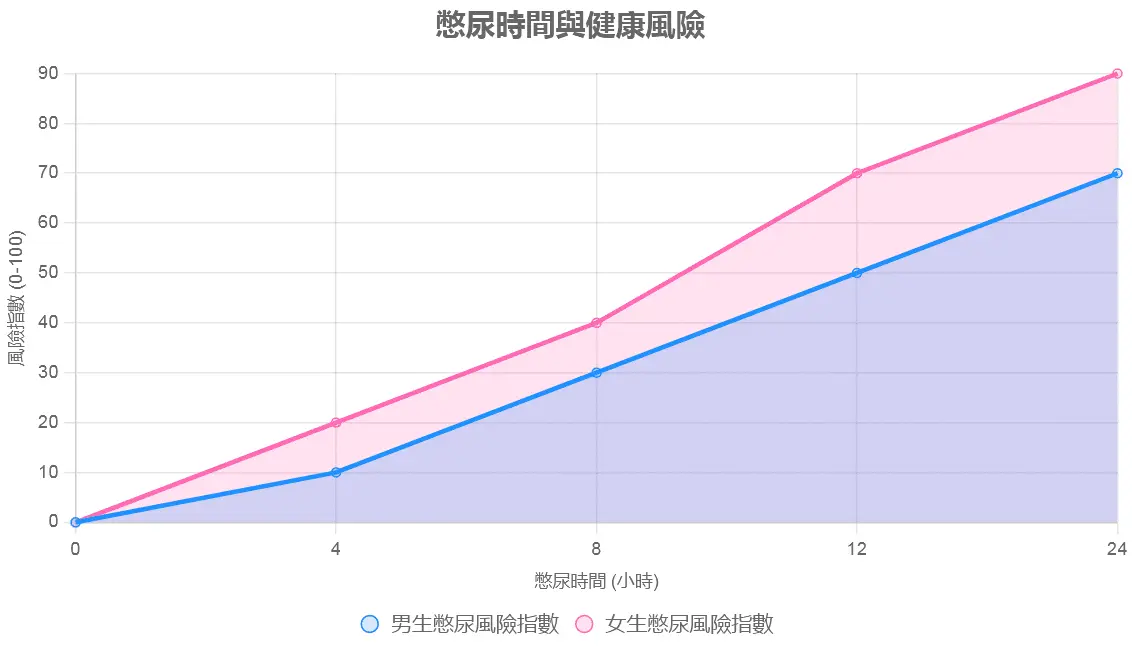
Cause Analysis:
The chart shows that the risk of bladder rupture increases sharply in women after holding urine for 8 hours due to muscle strength and urethral structure. The risk is even higher for women after 24 hours (although <1%) because of their lower bladder wall tolerance.
Prevalence of urinary incontinence and retention
describe:
This pie chart shows the prevalence of urinary incontinence and retention in men and women (%), categorized into stress incontinence, urge incontinence, and overflow incontinence:
- Boys(Blue series): Stress 3-11%, Urgency 40-80%, Overflow 5%.
- girl(Pink series): Stress 11-34%, Urgency 31%, Overflow 5%.
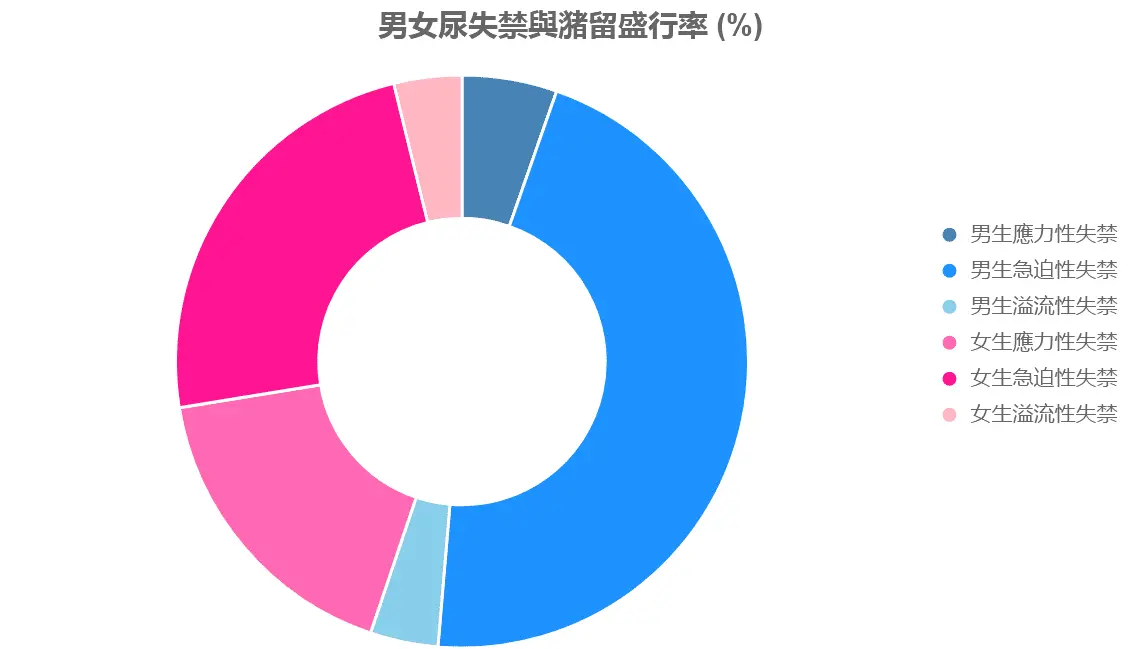
Cause Analysis:
The pie chart shows that the prevalence of stress incontinence is much higher in women (22.51 TP3T) than in men (71 TP3T), due to childbirth and estrogen influence. Urgency incontinence is higher in older men (prostate problems), while the overall incontinence rate in women (11.21 TP3T) is twice that in men.
in conclusion
Men's ability to "stop urinating instantly" stems from anatomical and hormonal advantages, but women can improve this through practice. While deaths from holding urine are rare, history and data confirm the risk. It is recommended to seek medical attention promptly and avoid forcibly holding urine.
Further reading:

-copy-300x225.webp)