





The profound impact of diabetes on male sexual function
Table of contents
"My performance in bed has been getting worse lately. Is it because I'm getting older?" Many men don't realize this.diabetesThis is the silent killer that leads to sexual dysfunction. Diabetes is closely related to men's sexual health, and its impact goes far beyond simple blood sugar problems, involving...Blood vesselThis article delves into how diabetes affects male sexual function on multiple levels, including the nervous, hormonal, and psychological aspects.Erectile dysfunction(ED), and through timelines and charts, analyzes the progression of the disease from its early to late stages, and finally provides practical management and treatment strategies.

Chapter 1: Understanding the Severity of the Problem – Let the Data Speak
The impact of diabetes on male sexual function should not be underestimated; the following data reveals its severity:
- The incidence rate is extremely high.The probability of erectile dysfunction in men with diabetes is lower than that in men without diabetes.3 timesabove.
- Early onset timeErectile dysfunction (ED) is typically more common in people with diabetes than in people without diabetes.10-15 years in advanceAppear.
- Related to the diseaseAs the duration of diabetes increases and glycemic control worsens, the incidence and severity of erectile dysfunction (ED) also increase. In patients with a disease duration of more than 10 years, the incidence of ED can be as high as [missing information - likely a percentage].70% and above.
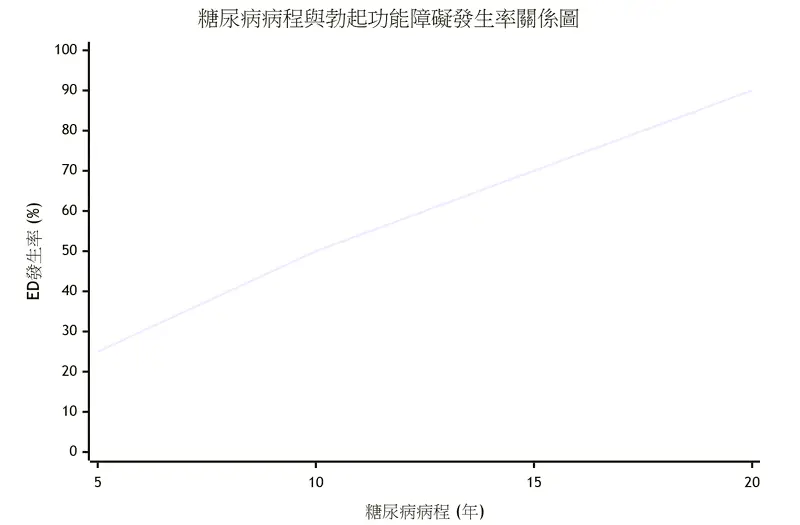
(This is a schematic diagram, combining data from multiple studies.)Despite the prevalence of this problem, many patients choose silence and avoidance due to societal expectations of masculinity and the privacy associated with the topic of sex. This not only delays medical treatment but also leads to secondary harm such as anxiety and depression, severely impacting their quality of life and relationships.

Chapter Two: How Diabetes Destroys Male Virility—Analysis of Multiple Mechanisms
Diabetes does not affect sexual function through a single pathway, but rather through a "comprehensive" attack pattern, with the following main mechanisms:
1. Vasculopathy – a key blood supply problem
An erection is essentially aVascular eventsWhen sexual stimulation occurs, the brain sends a signal, causing the arteries in the corpora cavernosa of the penis to dilate rapidly, allowing a large amount of blood to flow into the corpora cavernosa. At the same time, the veins are compressed to prevent blood from flowing out, thus achieving a firm erection.
- The damage caused by high blood sugarLong-term high blood sugar can damage vascular endothelial cells, preventing them from producing nitric oxide (NO) normally. Nitric oxide is essential for relaxing vascular smooth muscle and dilating arteries.Key Messenger.
- AtherosclerosisDiabetes accelerates atherosclerosis in blood vessels throughout the body, including the small arteries leading to the penis. The vessel walls thicken and harden, and the lumen narrows, leading to…Insufficient blood flowJust like a rusty water pipe that can't supply water smoothly, an erection is naturally difficult to achieve or cannot be maintained.
2. Neuropathy – Disruption of signal transmission
An erection requires a complete neural pathway: from the brain's sexual desire activation, to the spinal cord's reflex, and then the instruction is transmitted to the penis.
- High blood sugar can damage these peripheral nervesEspecially the tiny nerve fibers responsible for sensory and autonomic nervous functions. This leads to:
- Dull sensesDecreased sensitivity of the glans penis and penis reduces the intensity of sexual stimulation.
- Signal transmission failureThe "erection command" from the brain to the penis cannot be effectively delivered, and the erection process cannot be initiated.
3. Endocrine Dysfunction – Loss of Motivation
Testosterone is the male libido hormone.Main driving force.
- Research showsThe proportion of male patients with type 2 diabetes who also have hypogonadism (low testosterone) is significantly higher than that in the general population.
- High blood sugar and obesity(Especially central obesity) can affect the function of the hypothalamus-pituitary-gonadal axis, leading to a decrease in testosterone synthesis.
- Low testosteroneNot only directly causedDecreased libidoIt can also exacerbate insulin resistance and central obesity, creating a vicious cycle.

4. Psychological Factors – The Starting Point of a Vicious Cycle
Physical failure can easily trigger psychological problems, which in turn can worsen erectile dysfunction, creating a vicious cycle of "performance anxiety."
- First failureOccasional erectile dysfunction due to poor blood sugar control.
- Anxiety and fearThe patient begins to worry about their performance next time, developing anticipatory anxiety such as "What if I fail again this time?"
- Self-fulfillmentStress and anxiety cause the body to secrete adrenaline (noradrenaline), a hormone that...Strongly suppressAn erection response leads to another failure, further intensifying anxiety.
5. Drug side effects and other complications
- Some blood pressure medications (such as diuretics and beta-blockers) may have negative effects on sexual function.
- Common complications of diabetes, such as depression and cardiovascular disease, can also affect sexual function.
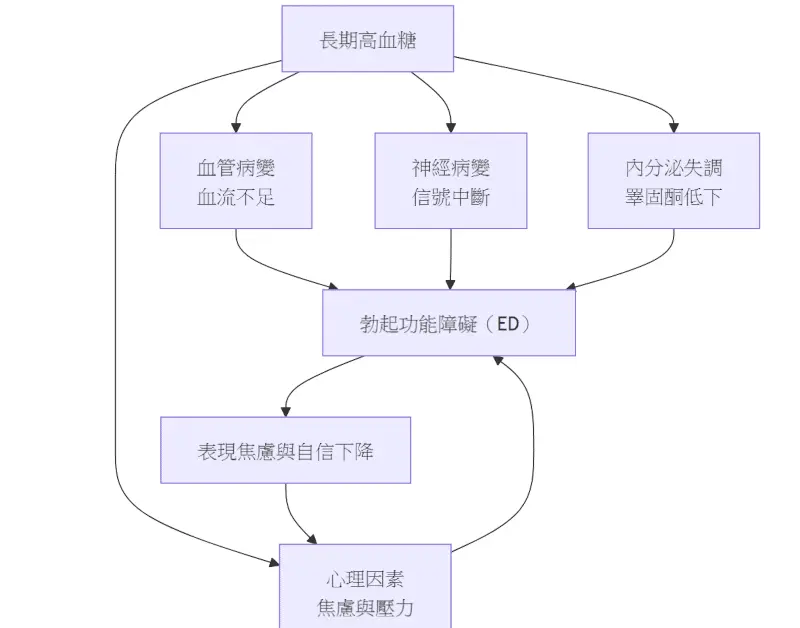
To better understand this multi-faceted attack, the following diagram illustrates its combined action path:
| stage | Average duration of illness | Main changes | Reversibility |
|---|---|---|---|
| Issue 0 | 0 years | Mild endothelial dysfunction | high |
| Phase 1 | 3–5 years | Nocturnal erection frequency decreased by 20 % | middle |
| Phase 2 | 5–10 years | Insertion success rate <60% % | Low |
| Phase 3 | >10 years | Unable to penetrate or completely unable to achieve an erection | extremely low |
Chapter 3: The Timeline of Diabetic Erectile Dysfunction – From Insidious to Obvious
The impact of diabetes on sexual function is a gradual and continuous deterioration, not something that happens overnight. The following diagram illustrates its typical developmental stages:
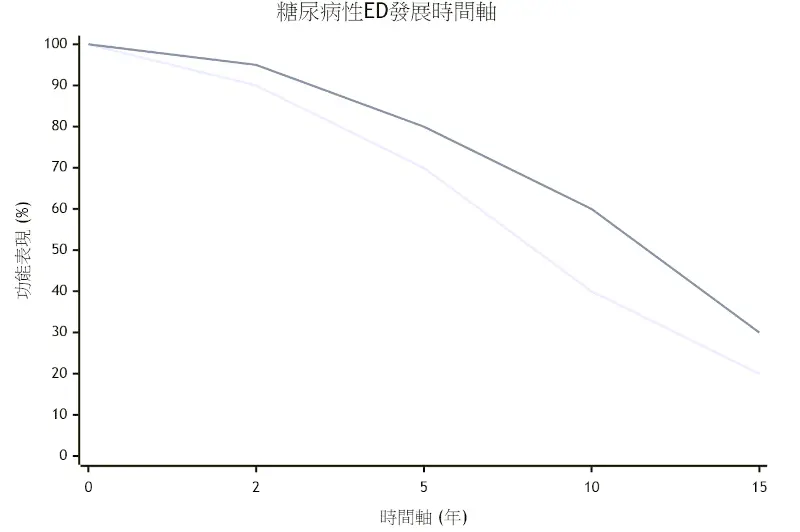
(This is for illustrative purposes only; individual differences may exist.)
Phase 1: Incubation period (0-5 years after diagnosis)
- Physiological changesHigh blood sugar has already begun to cause minor damage to blood vessels and nerves, but the body still has the ability to compensate.
- Clinical manifestationsPatients may experience no sensation at all, or only a slight decrease in erectile rigidity, and occasionally a feeling of "feeling powerless," but overall they can still complete sexual intercourse. This stage is the easiest to overlook, yet it is crucial.Golden period for intervention and prevention.
Phase Two: Gradual Developing Stage (5-10 years after diagnosis)
- Physiological changesVascular and nerve lesions worsen, arterial blood flow is significantly reduced, and nerve conduction velocity decreases.
- Clinical manifestationsThe erection is significantly less firm, requiring more direct and intense stimulation to achieve an erection. After erection...Difficult to maintain(The erection cannot be maintained), and it is easy to lose firmness midway. The success rate of intercourse begins to decline, and the patient begins to feel anxious.
Phase 3: Severe stage (more than 10 years after diagnosis)
- Physiological changesThe lesions in both large and small blood vessels are already quite severe, and nerve damage may be irreversible.
- Clinical manifestations:Complete or near-complete inability to achieve an erectionOral medications (such as PDE5 inhibitors) become less effective or even ineffective. Libido is also significantly reduced due to possible low testosterone levels. At this point, the problem has become more comprehensive, requiring more aggressive and integrated treatment.

Chapter 4: Diagnosis and Assessment – Finding the Specific Cause
If you suspect you have diabetic erectile dysfunction (ED), you should seek medical attention.UrologyorDepartment of Endocrinology and MetabolismThe assistance of a physician. Diagnosis typically includes:
- Detailed consultationUnderstand the patient's medical history, medication history, and psychosocial factors.
- Physical examinationExamine secondary sexual characteristics, external genitalia, and peripheral vascular pulsation.
- Laboratory tests:
- Blood sugar relatedGlycated hemoglobin (HbA1c) and fasting blood glucose.
- HormonesTotal testosterone, free testosterone, prolactin, and luteinizing hormone (LH).
- Blood lipids and thyroid function.
- Special examination (if necessary):
- Nocturnal penile tumescence test (NPT)Distinguish between psychogenic and organic erectile dysfunction (ED).
- Doppler ultrasound: Assess the blood flow status of the pudendal artery.
Chapter 5: Comprehensive Management and Treatment Strategies – Regaining a Happy Sexual Life
Treatment of diabetic erectile dysfunction requires a multi-pronged approach; relying solely on aphrodisiacs has limited effectiveness.
Strategy 1: The fundamental solution – strict blood sugar control
- TargetControlling glycated hemoglobin (HbA1c) within a certain range7% and below(As determined by the physician based on individual circumstances).
- importanceThis is the foundation of all treatments. Stabilizing blood sugar can...Slow down or even partially reverseTo prevent the progression of vascular and nerve diseases and curb the worsening of the problem at its root.

Strategy Two: First-line oral medications – PDE5 inhibitors
- Common drugs: Sildenafil, Tadalafil, Vardenafil.
- Working principleThese are not "aphrodisiacs," but rather enhance the vasodilatory effect of nitric oxide (NO) by inhibiting the PDE5 enzyme, thereby improving erectile function.
- Important Notice:
- Need for sexual stimulationThe drug itself does not induce an erection; sexual stimulation is still required to initiate it.
- Not effective for everyoneFor patients with severely damaged blood vessels, the effect may be poor.
- Use under the guidance of a physician.Especially for patients with underlying heart disease.
Strategy 3: Hormone Replacement Therapy – Targeting Low Testosterone
- If tests confirm that testosterone levels are too low, the doctor may recommend testosterone supplementation (gel, injection, etc.).
- benefitIt can effectively enhance libido, improve mood and physical performance, and may have an auxiliary effect on blood sugar control.

Strategy 4: Second-line treatment options
When oral medications are ineffective, there are still other options:
- Vacuum suction device (VCD)This method uses negative pressure to draw blood into the penis and uses a clamping ring to maintain an erection. It is a non-invasive and effective physical therapy.
- Intracavernosal injection (ICI) of medication into the penis.Injecting vasodilators directly into the penis yields a powerful and rapid effect.
- Ureteral suppositories (MUSE)Tiny pills are placed at the urethral opening, and the drug is absorbed through the urethra to induce an erection.
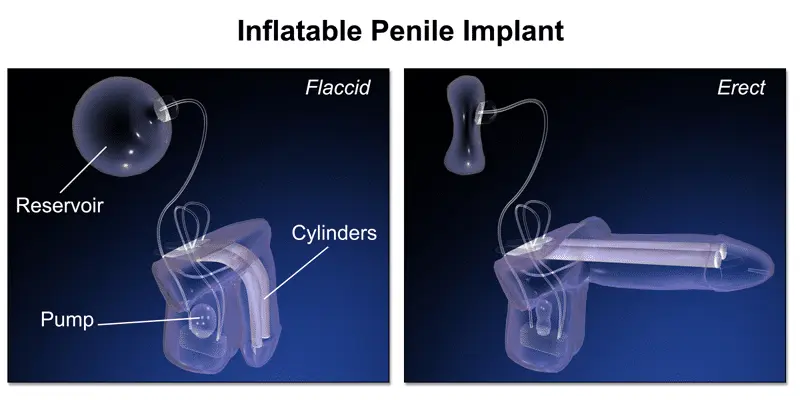
Strategy Five: The Last ResortPenis implantation
- For severely ill patients for whom all other treatments have failed, this is the final andExtremely high satisfaction rateThe solution.
- Through surgery, an inflatable device is implanted in the penis, allowing the patient to initiate an erection when needed and return to normal after sexual intercourse. The success rate is as high as 95% (TP3T or higher).

Strategy Six: Lifestyle Adjustment – The Foundation of All
- sportsAim for at least 150 minutes of moderate-intensity aerobic exercise (such as brisk walking or swimming) plus two strength training sessions per week. Exercise can improve blood flow, increase insulin sensitivity, and boost testosterone.
- dietAdopt the Mediterranean diet (rich in fruits, vegetables, whole grains, and healthy fats) and control the total amount and quality of carbohydrates.
- weight lossReducing body fat, especially visceral fat, can significantly improve hormone levels and blood sugar.
- Quit smoking and limit alcohol consumptionSmoking severely damages blood vessels, while alcohol inhibits nerve responses.

Strategy Seven: Communication and Psychological Support with Partners
- Open communication: Have an open and honest conversation with your partner about your difficulties and feelings, so that they understand that this is an "illness" rather than "lack of love" or "lack of attraction." Facing problems together can reduce stress and enhance intimacy.
- Seeking professional helpIf necessary, seek assistance from a sex therapist or psychologist to address performance anxiety and relationship issues.
| hierarchy | plan | Level of evidence | Expected improvement in IIE F-5 |
|---|---|---|---|
| Base | Blood sugar control, exercise, Mediterranean diet | A | +3–4 points |
| First line | PDE5 inhibitors (sildenafil, tadalafil) | A | +6–8 points |
| Second-tier | Vacuum negative pressure device, sponge injection PGE1 | B | +4–6 points |
| Third line | Inflatable penile prosthesis | B | 90% success rate % |
| Support | Testosterone supplementation (TT <8 nmol/L) | A | +5–7 points |

in conclusion
The impact of diabetes on male sexual function is comprehensive and far-reaching. Through a chain reaction involving blood vessels, nerves, hormones, and psychology, it silently erodes men's confidence and intimate relationships. However, this is by no means an incurable disease or a fate to be silently endured.
Most importantlyBreak the silenceFacing the problem head-on is the first step to solving it. Actively discuss it with your doctor, undergo a comprehensive evaluation, and understand the exact cause behind it. Treatment must begin with...Strictly control blood sugarStart by addressing the root cause, and combine this with multiple strategies such as lifestyle adjustments, medication, and partner support.
Sexual function is an important indicator of overall health, and diabetic erectile dysfunction (ED) can be an early warning sign of cardiovascular disease. Therefore, paying attention to your "performance in bed" is essentially paying attention to your "heart" and "vascular" health. Through proactive management, you not only have the opportunity to regain a fulfilling sex life, but also to achieve a more comprehensive and lasting healthy future.
Further reading:
{kind=link}
{kind=link}