




[Video] The relationship between blood vessels and male erections
Table of contents
Erectile function—a topic long shrouded in shame and silence, yet crucial to the physical and mental health and quality of life of countless men. As night falls and the bedroom becomes a silent battlefield, many men face an unspeakable predicament: the penis cannot achieve or maintain sufficient rigidity. Society often attributes this to "kidney deficiency," "age," or "psychological stress," neglecting a vital physiological truth: the essence of erectile function is a delicate process...Blood vesselevent.
Modern medical research has clearly revealed that in over 80% of cases of erectile dysfunction (ED), the root cause is not simply psychological factors or the mysterious "kidney deficiency," but rather...Health status of the vascular systemPenile erection is essentially a highly coordinated hemodynamic performance, a symphony composed by blood vessels, nerves, and endothelial cells. This means that the seemingly simple penis actually becomes an "early warning system" for the overall vascular health of men, a natural "vascular health detector."
Erectile Mechanism
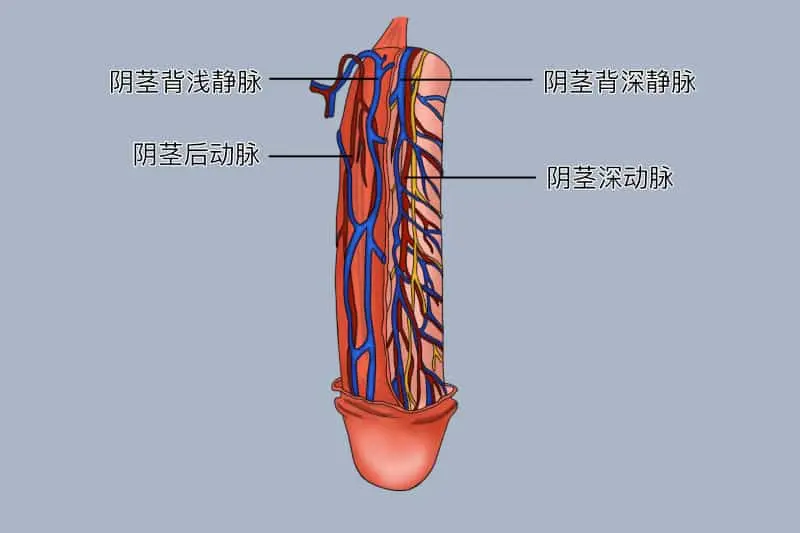
To understand erectile function, one must first understand...penisThe penis has a unique structure. It is mainly composed of three columnar corpora cavernosa: two corpora cavernosa of the penis and one corpus spongiosum of the urethra. These spongy tissues are not solid muscles, but a complex network of countless tiny sinusoids, similar to a highly specialized vascular sponge.
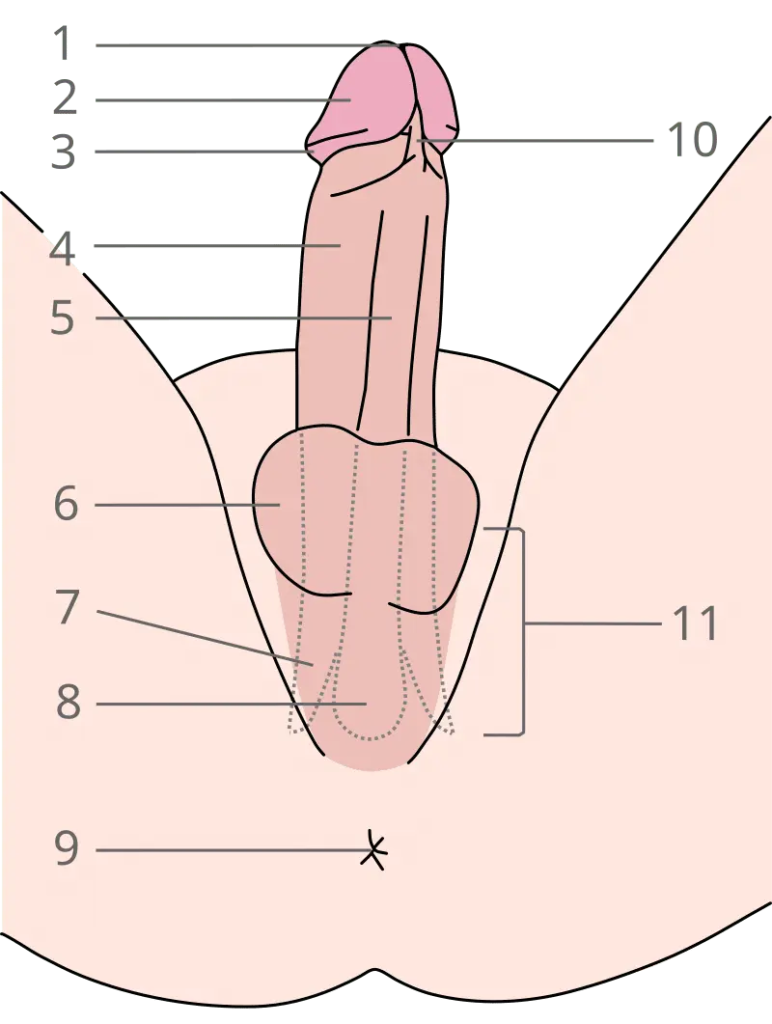
Structure of the penis (urethral surface, erect state): 1.external urethral meatus 2.glans penis 3.coronal sulcus 4.Corpus cavernosum of the penis 5. Corpus spongiosum 6.scrotum 7.Penis crest 8. Urethral bulb 9.anus 10.Frenulum 11.Penis root
When sexual stimulation occurs, the brain and local nerves send signals, initiating an amazing...Blood vesselchange:
- Release of vasodilatory signalsNerve endings release nitric oxide (NO)—the most important signaling molecule during erection. Nitric oxide diffuses to the smooth muscle cells of the corpus cavernosum, activating guanylate cyclase, leading to an increase in cyclic guanosine monophosphate (cGMP) levels, which in turn causes smooth muscle relaxation.
- Arterial blood flow surgeThe relaxed smooth muscle causes the penile arteries to dilate dramatically, increasing blood flow from approximately 4 ml per minute at baseline to 80-120 ml per minute, a 20-30 fold increase. This surge of blood floods into the network of vascular sinuses within the corpus cavernosum.
- Activation of venous occlusion mechanismAs the cavernous sinuses become congested and swell, they exert pressure on the tunica albuginea (a tough fibrous membrane). This pressure compresses the emissary veins that emerge from the tunica albuginea, effectively "closing" the blood flow channel, similar to pinching the outlet of a water pipe with your fingers.
- The final stage of a firm erectionThe continuous inflow of blood and the near cessation of outflow cause the pressure inside the penis to surge to near systolic blood pressure (approximately 100 mmHg), thus achieving the rigidity required for a full erection. At this time, the oxygen partial pressure within the corpora cavernosa rises from 20-40 mmHg at rest to 100 mmHg, fully reaching the level of arterial blood.
This delicate physiological process depends entirely on the health of the vascular system. Any factor that affects vascular function, blood flow, or nerve signal transmission can disrupt this intricate chain, leading to erectile dysfunction.
Endothelial cells: gatekeepers of vascular health and key regulators of erection
The inner wall of blood vessels is covered by a thin but powerful layer of cells—endothelial cells. This inner membrane, composed of only a single layer of cells, is the "gatekeeper" of the health of blood vessels throughout the body and a key regulator of erectile function.
Endothelial cells regulate vascular tone by producing a variety of vasoactive substances, the most important of which is nitric oxide (NO). Healthy endothelial cells produce sufficient nitric oxide to ensure that blood vessels can dilate adequately when needed. However, when endothelial function is impaired, nitric oxide production decreases while degradation increases, and excessive production of vasoconstrictors such as endothelin-1 may also occur, leading to ineffective vasodilation.
Studies show that the endothelial cells within the corpora cavernosa of the penis are particularly crucial for erectile function. They not only respond to the release of nitric oxide from nerves, but also produce nitric oxide themselves under the shear force of blood flow, further enhancing the erectile response. This explains why maintaining endothelial health is so important for erectile function.
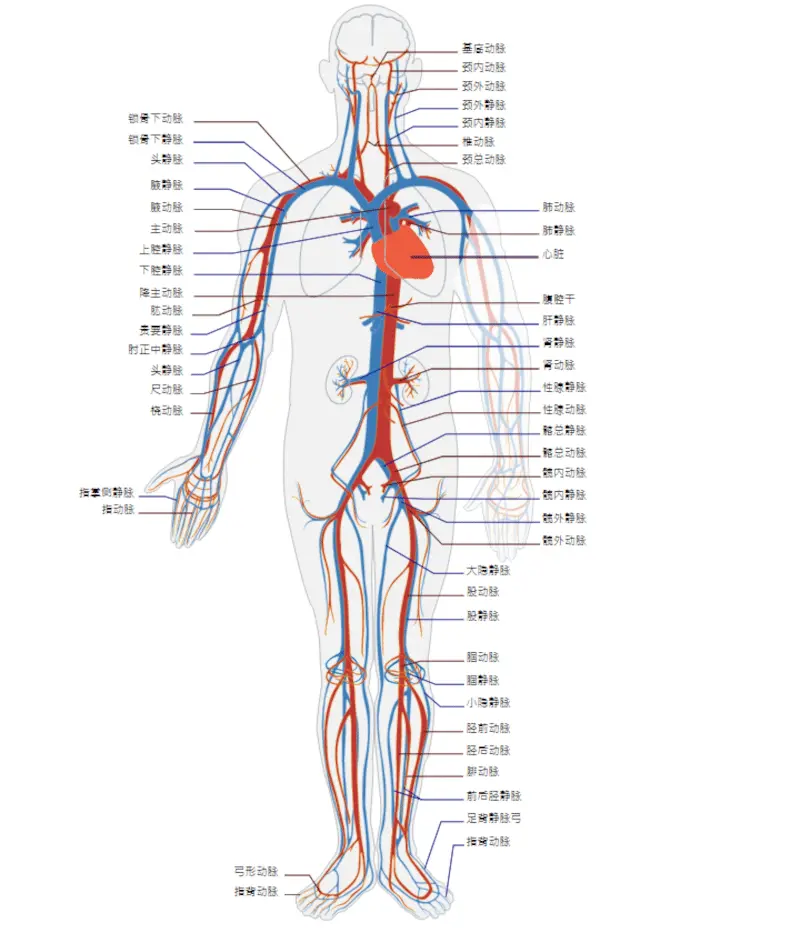
Multiple studies have confirmed that patients with erectile dysfunction (ED) often exhibit hallmarks of systemic endothelial dysfunction, such as impaired blood flow-mediated vasodilation. This reinforces the view that ED serves as an early warning sign of cardiovascular disease: penile vessels may show functional abnormalities earlier than the coronary arteries or carotid arteries, partly because penile arteries are smaller in diameter (1-2 mm, compared to 3-4 mm in the coronary arteries) and more sensitive to changes in blood flow.

Erectile dysfunction as an early warning system for cardiovascular disease
The view that "the penis is a barometer of cardiovascular health" has been widely accepted in the medical community. In fact, erectile dysfunction often occurs 2-5 years before obvious cardiovascular symptoms (such as chest pain and shortness of breath) appear, providing a valuable early warning window for preventing major cardiovascular events.
This time lag has a physiological basis: smaller blood vessels (such as the penile artery) are more prone to blockage due to atherosclerosis than larger vessels. When the penile artery experiences a blockage of 501 TP3T, erectile function may be affected; however, the same degree of blockage in a larger coronary artery may not cause obvious symptoms. Only when the coronary artery blockage reaches 701 TP3T or more will typical angina symptoms appear.
This discovery has significant clinical implications:Erectile dysfunction may be a "canary in the coal mine," indicating a future risk of cardiovascular events.Multiple large-scale epidemiological studies support this view:
- A prospective study of men aged 40-70 found that, after adjusting for age, men with erectile dysfunction (ED) had a 1.5 times higher risk of developing coronary heart disease than men without ED.
- Another study showed that patients with erectile dysfunction (ED) have an increased combined risk of future myocardial infarction, stroke, or peripheral artery disease (45%).
- Patients with diabetes and erectile dysfunction (ED) have a significantly higher cardiovascular mortality rate than diabetic patients without ED.
Therefore, erectile dysfunction in men should not be viewed merely as an isolated sexual dysfunction, but rather as a warning sign for a comprehensive assessment of cardiovascular health. Clinicians now often refer to ED as a "sentinel of vascular dysfunction" and recommend comprehensive screening for cardiovascular risk factors in ED patients.

Risk factors that damage vascular health and erectile function
Several risk factors can impair vascular function, thereby affecting erectile function. Understanding these factors can help in taking targeted preventative measures.
1. Age factor
Age is one of the strongest contributing factors to erectile dysfunction (ED). With increasing age, endothelial function naturally declines, nitric oxide bioavailability decreases, the amount of smooth muscle in the corpora cavernosa decreases while fibrosis increases, and arterial compliance decreases. Studies show that the prevalence of ED in men over 40 is approximately 401 TP3T, rising to 701 TP3T in those over 70. However, age itself should not be viewed as an inevitable fate; many older men maintain good erectile function by actively managing other risk factors.

2. Cardiovascular disease and metabolic syndrome
Hypertension, hyperlipidemia, diabetes, and obesity are collectively known as components of metabolic syndrome, which impair vascular function through multiple mechanisms:
- Hypertension: Sustained high blood pressure damages the vascular endothelium, and many antihypertensive drugs (especially beta-blockers and thiazide diuretics) may worsen erectile dysfunction (ED).
- High blood lipids: Low-density lipoprotein cholesterol is oxidized and then engulfed by macrophages to form foam cells, initiating the process of atherosclerosis.
- Diabetes: High blood sugar leads to the accumulation of advanced glycation end products (AGEs), causing oxidative stress and endothelial dysfunction. Men with diabetes have a 3-4 times higher risk of developing erectile dysfunction (ED) than non-diabetic individuals, and the onset age is also earlier.
- Obesity: Adipose tissue, especially visceral fat, produces inflammatory factors and leptin, reducing nitric oxide synthesis. Obesity is also often accompanied by decreased testosterone levels.
3. Smoking and alcohol
Nicotine and other toxins in tobacco directly damage vascular endothelium, promote oxidative stress and inflammation, and accelerate atherosclerosis. Studies have shown that smokers have a 1.5-2 times higher risk of developing erectile dysfunction (ED) than non-smokers, and this risk is dose-dependent. Excessive alcohol consumption affects erectile function through multiple mechanisms, including central nervous system suppression, direct testicular toxicity leading to decreased testosterone levels, and inducing peripheral neuropathy.
4. Psychological stress and lack of exercise
Chronic stress leads to overactivation of the sympathetic nervous system, releasing excessive catecholamines that cause vasoconstriction. Simultaneously, stress-related increases in cortisol can suppress testosterone production. Lack of exercise results in decreased cardiovascular adaptability, impaired endothelial function, and is often associated with obesity and metabolic problems.
5. Medications and other medical conditions
Many commonly used medications can affect erectile function, including antihypertensive drugs, antidepressants (especially SSRIs), antipsychotics, antihistamines, and hormone preparations. In addition, pelvic surgery (such as radical prostatectomy), radiation therapy, and neurological diseases (such as multiple sclerosis and Parkinson's disease) can also damage the neurovascular structures related to erection.

Assessment and Diagnosis: Erectile Function as a Perspective on Systemic Vascular Health
When men raise concerns about erectile function, a comprehensive medical evaluation is crucial, not only to address sexual function issues but also as an opportunity to assess overall cardiovascular health.
Clinical assessment should include:
- Detailed medical history taking: including the nature of the erectile problems, the time of onset, situational specificity (whether an erection can still be achieved under certain circumstances), and related cardiovascular symptoms.
- Risk factor assessment: A comprehensive assessment of cardiovascular risk factors, including smoking, diet, exercise habits, family history, etc.
- International Index of Erectile Function (IIEF) Questionnaire: A Standardized Tool for Quantifying the Severity of Erectile Dysfunction
- Physical examination: including examination of the cardiovascular system, secondary sexual characteristics, peripheral vascular pulsation, and nervous system.
- Laboratory tests: fasting blood glucose and glycated hemoglobin (HbA1c), lipid profile, total testosterone and free testosterone levels, luteinizing hormone (LH), and prolactin (if necessary).
Special examinations may include:
- Nocturnal penile tumescence test (NPT): Differentiating between psychogenic and organic erectile dysfunction (ED)
- Doppler ultrasound examination: assesses penile arterial blood flow, and measures peak systolic velocity (PSV), end-diastolic velocity (EDV), and resistance index (RI).
- Cavernosal manometry and angiography: More invasive procedures, usually reserved for complex cases or patients scheduled for vascular surgery.
Importantly, the assessment of patients with erectile dysfunction (ED) should not stop at the penis itself, but should be viewed as a window into assessing overall vascular health. Many experts recommend cardiovascular risk stratification for ED patients, determining further cardiovascular examinations (such as exercise stress testing, coronary CT angiography, etc.) based on the risk level.

Comprehensive strategies for improving vascular health and erectile function
The key to improving erectile function lies in improving vascular health, which requires a comprehensive and multi-dimensional strategy.
1. Lifestyle intervention: the foundation of all interventions
- Physical activity: At least 150 minutes of moderate-intensity or 75 minutes of vigorous-intensity aerobic exercise (such as brisk walking, running, or swimming) per week can significantly improve endothelial function. Studies have shown that regular exercise can reduce the severity of erectile dysfunction by 40-60%.
- Dietary adjustments: The Mediterranean diet (rich in fruits, vegetables, whole grains, olive oil, and fish) is associated with better vascular function and erectile function. Particularly recommended foods include flavonoid-rich berries, dark chocolate, watermelon (containing citrulline, a precursor to nitric oxide), and nuts.
- Weight management: Weight loss of 5-101 TP3T can significantly improve erectile function, partly by reducing inflammation and improving insulin sensitivity.
- Quit smoking and limit alcohol consumption: After quitting smoking, vascular function gradually improves, reducing the risk of erectile dysfunction (ED). Alcohol consumption should be limited to 1-2 standard drinks per day.
2. Risk factor control
Strictly control blood pressure (<130/80 mmHg), blood lipids (LDL-C to target level according to risk level), and blood glucose (HbA1c <7% for diabetic patients). Choose antihypertensive drugs with minimal impact on erectile function (such as angiotensin receptor blockers (ARBs) and calcium channel blockers).
3. Psychological and Relational Factors
For erectile dysfunction (ED) with psychological factors, cognitive behavioral therapy and couples counseling may be helpful. Stress management techniques (such as meditation and deep breathing exercises) can reduce sympathetic nerve tone and improve erectile response.
4. Drugs and Medical Interventions
- Phosphodiesterase 5 inhibitors (PDE5i): such asSildenafil(Viagra)TadalafilDrugs like Cialis, which enhance the effect of nitric oxide by inhibiting cGMP degradation, are the first-line treatments. Note that these drugs are "enhancers," not "stimulants," and require sexual stimulation to be effective.
- Testosterone replacement therapy: only applicable to patients diagnosed with testosterone deficiency, and requires monitoring of prostate-specific antigen (PSA) and hematocrit.
- Vacuum Erection DeviceMechanical negative pressure causes penile engorgement, suitable for patients who cannot use medication.
- Intracavernosal injection: Direct injection of vasoactive drugs (such as prostaglandin E1) into the penis, with an efficacy rate of 80-90%.
- Vascular surgery and implants: For severe arterial or venous ED, vascular reconstruction surgery or penile prosthesis implantation may be considered.
5. Emerging Therapies and Future Directions
The new therapies under investigation include:
- Low-energy shockwave therapy: Improves erectile function by stimulating angiogenesis and nerve regeneration.
- Stem cell therapy: potentially repairs damaged corpus cavernosum tissue through multiple mechanisms.
- Gene therapy: aims to enhance nitric oxide synthesis or the expression of other vasoactive substances.
Further reading:


